

-
 Written By:
Alex Herrera
Written By:
Alex Herrera
-
Edited By:
Christina Holmes
-
Clinically Reviewed By:
Dr. Ash Bhatt, MD, MRO
 Written By:
Written By:
 Edited By:
Edited By:
 Clinically Reviewed By:
Clinically Reviewed By:
She didn’t see it coming. The prescription was for anxiety disorder, a small white pill, a reasonable expectation that things would ease. And for a while, they did. But somewhere along the way, manageable became dependent, and a low, persistent feeling of depression started emerging beneath the anxiety the medication had been suppressing. Maybe it was always there. Maybe the medication created it. Probably both.
This is the story we hear most often from the people who come to Legacy Healing New Jersey seeking help for what their doctor initially called an anxiety disorder, but what has quietly become something more complicated: a co-occurring condition or dual diagnosis.
Research consistently shows that more than half of people with a substance use disorder also meet criteria for at least one co-occurring mental health condition. Benzodiazepines and depression are among the most common pairings, and among the most undertreated.
This article explains why these two conditions so frequently appear together, why treating one without the other almost guarantees relapse, and what integrated treatment for Xanax addiction and depression actually looks like in practice.
Key Takeaways
|
Why Xanax Dependence and Depression Frequently Occur Together
Xanax addiction and depression share deep neurological roots. Understanding that connection is the first step toward understanding why integrated treatment is essential.
1. It Starts With How Benzodiazepines Change the Brain
Benzodiazepines like Xanax work by enhancing the effect of GABA, the brain’s primary inhibitory neurotransmitter. A GABA imbalance causes the brain’s threat-detection system to run hot, and Xanax works rapidly and effectively by amplifying GABA’s calming signal.
The problem starts when the brain begins downregulating its own GABA production due to an artificial GABA boost. After a few weeks and months, the baseline GABA level drops, and the medication that once worked is now simply maintaining a system that has become dependent on Xanax.
2. Then, Rebound Depression Sets In as Tolerance Grows
As tolerance builds, the medication that was prescribed to reduce anxiety begins generating its own mood instability. Between doses, the person doesn’t return to their pre-medication baseline; they fall below it. The brain, habituated to the drug’s GABA enhancement, experiences its absence as an acute deficit.
This rebound effect first feels like anxiety, but it deepens, over time, into a persistent low mood and a sense of flatness that doesn’t respond to circumstances. This is not the original anxiety disorder. This is benzodiazepine-induced depressive disorder, and it will not resolve without addressing benzodiazepine dependence that’s driving it.
3. Until Each Dose Deepens the Cycle of Crash and Relief
The cruelest aspect of long-term benzodiazepine dependence is that it creates the very suffering it appears to relieve.
Many people describe this phase as chasing a feeling of normalcy that keeps moving further away. They are not imagining it. The neurological normal has genuinely shifted, and will require carefully managed care to re-establish.
Quick Answers from Dr. Ash Bhatt
“What I want patients to understand is that this is not two separate problems, it’s one interconnected neurological cycle. Xanax changes how the brain regulates calm and mood over time, and what initially relieves anxiety can eventually create a deeper depressive state. That’s why treating both together is not optional, it’s essential.”
When Anxiety Medication Use Becomes a Dual Diagnosis Condition
A co-occurring mental health and substance use disorder, is present when both a psychiatric condition and a substance use disorder exist independently, each requiring its own treatment. They are mutually sustaining, mutually worsening, and mutually resistant to single-track treatment.
The benzodiazepine addiction symptoms and signs of dual diagnosis in the context of Xanax and depression typically include:
- Benzodiazepine dependence symptom: using Xanax in amounts greater than prescribed, or for longer than intended
- Continued use despite recognizing that the medication is worsening mood or functioning
- Unsuccessful attempts to reduce or stop use
- Physical withdrawal symptoms when the drug is delayed or absent, including heightened anxiety, sweating, tremor, or insomnia
- A persistent depressive mood that does not improve during periods of reduced use
- Social withdrawal, loss of interest in previously meaningful activities
- Cognitive changes: difficulty concentrating, memory problems, emotional blunting
Many of these symptoms overlap with the original anxiety disorder, which is precisely why professional clinical evaluation from our addiction experts is essential, rather than self-diagnosis.
What Standard Detox Misses And Why It Matters for This Condition
Standard detoxification programs are designed to manage withdrawal safely, and for many substances, that is sufficient as a starting point, but for benzodiazepine dependence co-occurring with depression, it is not.
For co-occurring Xanax dependence and depression, these are not the same treatment, and the difference determines long-term outcomes.
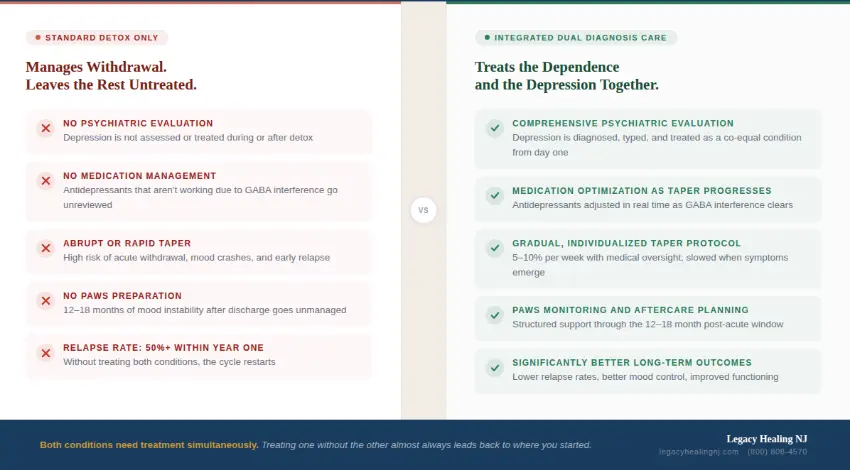
Detox treats the body’s physical dependency. It does not treat the neurological, psychological, or emotional conditions that both preceded and were created by that dependency. Without integrated psychiatric care, detox is the beginning of a cycle, not the end of one.
Why Treating Depression Without Addressing Xanax Use Increases Relapse Risk
Many people experiencing the depression-and-Xanax cycle first present to mental health care rather than addiction treatment, and may receive antidepressant therapy without any clinical attention to the benzodiazepine use. This is where relapse risk is most dangerously underestimated.
1. First, Antidepressants Stop Working Properly
Antidepressants depend on neurological stability to work. During active benzodiazepine dependence, that stability is absent. The GABA dysregulation directly interferes with the serotonergic and dopaminergic pathways antidepressants target, producing masked depression symptoms that persist despite adequate prescribing. The person experiences this as confirmation that their depression is untreatable, which deepens hopelessness and increases relapse risk.
2. Then, Stopping Becomes Its Own Crisis
The Xanax withdrawal timeline for short-acting benzodiazepines begins within 6–12 hours of the last dose, peaking at 24–72 hours. Alongside severe anxiety and insomnia, withdrawal-induced depression emerges, neurochemically distinct from the baseline mood disorder, acute, and intense. Without clinical management, this mood crash is the primary driver of early relapse.
After acute withdrawal resolves, many people experience post-acute withdrawal syndrome (PAWS): persistent low mood, anhedonia, sleep disruption, and cognitive fog lasting 12–18 months. Long-term mood instability during this window is a major driver of late relapse risk, and one of the strongest arguments for sustained structured aftercare.
3. And Quitting Without Support Carries Serious Risks
Abrupt Xanax discontinuation can produce severe emotional dysregulation beyond anxiety and depression, panic, rage, dissociation, and significant suicidal ideation risk are documented in the clinical literature. This is why benzodiazepine dependence should never be managed through unsupported self-discontinuation, and why integrated addiction treatment is the only appropriate framework for this population.
Quick Answers from Dr. Ash Bhatt
“One of the most common patterns I see is patients being treated for depression while the underlying benzodiazepine dependence is still active. In those cases, treatment often feels ineffective, not because it is, but because the root issue hasn’t been addressed. Without treating both conditions together, relapse risk remains high.”
What an Integrated Dual Diagnosis Treatment Model Actually Looks Like
Dual diagnosis rehab is not simply addiction treatment with a therapy component added. It is a fundamentally different clinical framework in which psychiatric and substance use treatment are designed and delivered as a unified system.
At Legacy Healing New Jersey, integrated addiction treatment for co-occurring Xanax dependence and depression involves several concurrent components, each calibrated to the individual’s clinical presentation.
Gradual Benzodiazepine Taper Under Medical Supervision
The foundation of safe treatment is medically supervised detox through a gradual benzodiazepine taper, a controlled dose reduction over weeks to months, allowing the nervous system to recalibrate. A common approach converts the current benzodiazepine to a longer-acting agent such as diazepam, producing a smoother reduction curve. Taper rates are individualized, typically 5–10% per week, with flexibility to slow based on symptom emergence.
Psychiatric Evaluation That Reflects the Actual Clinical Picture
A comprehensive psychiatric evaluation at intake creates a baseline for medication management that reflects the person’s actual neurological state, not their presentation during active dependence. As the taper progresses and masked depression symptoms emerge more clearly, antidepressant adjustments are made systematically. The goal is a stable, effective psychiatric regimen that supports long-term recovery without creating new dependencies.
Evidence-Based Therapy That Addresses Both Conditions
Pharmacological stabilization is necessary but not sufficient. The cognitive, behavioral, and emotional patterns that sustain both conditions require direct therapeutic attention.
- Cognitive Behavioral Therapy (CBT) addresses distorted thinking patterns common to both: catastrophizing, core beliefs about being unable to cope without medication, and the cognitive architecture of hopelessness.
- Dialectical Behavioral Therapy (DBT) builds skills in distress tolerance and emotional regulation, the precise capabilities most compromised by long-term benzodiazepine dependence.
Learn more about our holistic approach to healing.
Levels of Care That Step Down as Stability Grows
A Partial Hospitalization Program (5–6 hours per day, 5 days per week) provides maximum structure during acute stabilization. As stability progresses, our Intensive Outpatient Program (9–15 hours per week) allows gradual reintegration into daily life while maintaining the therapeutic infrastructure of recovery. The step-down from PHP to IOP to standard outpatient mirrors the neurological stabilization timeline.
Quick Answers from Dr. Ash Bhatt
“Effective treatment requires a coordinated approach. What we focus on is gradually stabilizing the nervous system through a supervised taper while simultaneously addressing mood, behavior, and underlying psychological factors. When both conditions are treated together, recovery becomes far more sustainable.”
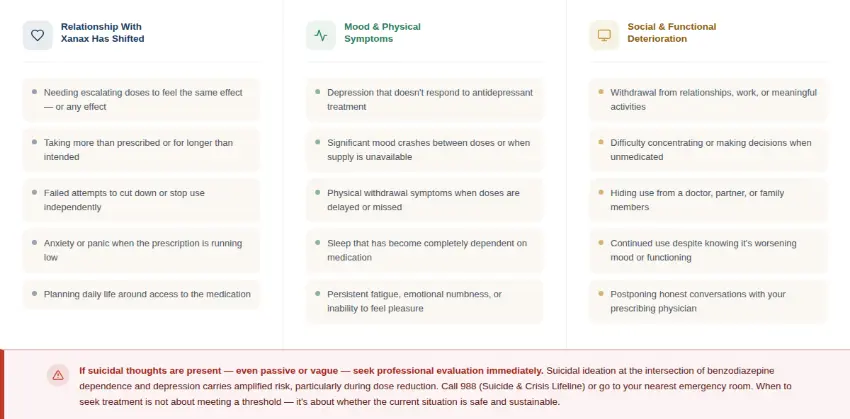
Warning Signs That Professional Dual Diagnosis Care Is Needed
These patterns are often subtle before they become acute. If several feel unfamiliar, that recognition matters, it’s a starting point, not a verdict.
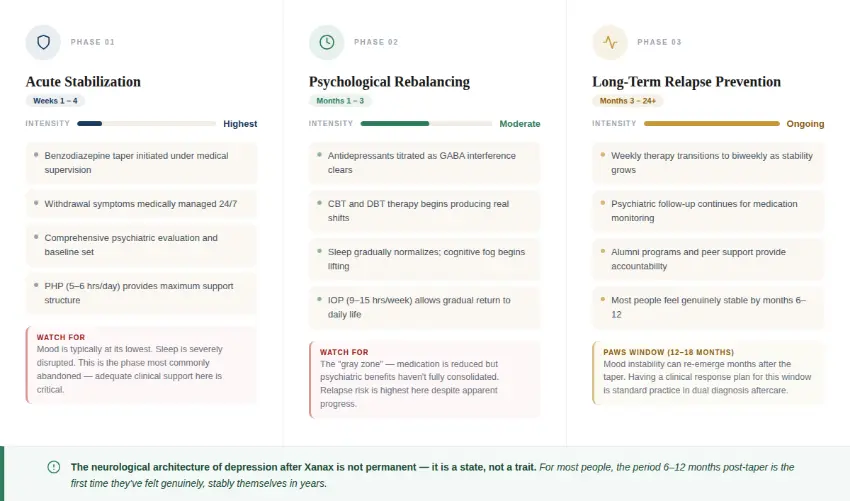
How Long Does Recovery From Benzodiazepine Dependence and Depression Take?
Recovery from co-occurring Xanax dependence and depression is a three phased, multi-month journey. Understanding the phases of the dual diagnosis recovery process helps set expectations that support rather than undermine progress.
Why Structured Treatment Improves Long-Term Mental Health Outcomes
People who receive simultaneous, coordinated treatment for both co-occurring conditions show consistently better outcomes across multiple measures: lower relapse rates, better psychiatric symptom control, improved social functioning, and higher rates of sustained employment.
The mechanism is straightforward: integrated treatment creates a clinical environment where progress on one front is immediately visible in its impact on the other. When mood destabilizes during the taper, the psychiatric and addiction teams respond together. When therapy reveals a cognitive pattern driving craving, the prescribing clinician is part of the same conversation.
Aftercare and psychiatric follow-up are not optional components of relapse prevention; they are its foundation. The clinical literature on sustained recovery from co-occurring disorders consistently identifies ongoing professional support, not willpower, not peer support alone, not time, as the most reliable predictor of long-term stability.
Can Depression Actually Improve After Stopping Xanax?
Yes, and for most people, significantly. Depression after Xanax is not permanent. As brain chemistry stabilization occurs, the suppressed GABA system recovering, serotonin and dopamine systems normalizing, the neurological substrate of depression begins to change.
Recovery from benzodiazepine dependence also dramatically improves therapy responsiveness. The antidepressants that seemed ineffective during active dependence frequently begin working once the neurological interference is removed. Many people describe 6–12 months post-taper as the first time they have felt genuinely, stably themselves in years.
Quick Answers from Dr. Ash Bhatt
“Yes, and this is something I emphasize often, depression after Xanax is not permanent. As brain chemistry begins to stabilize, many patients experience a significant improvement in mood. With the right support, people often feel more like themselves than they have in years.”
The First Step Is a Clinical Conversation
At Legacy Healing New Jersey, we specialize in integrated treatment for co-occurring disorders, including Xanax dependence and depression. Our clinical team conducts comprehensive dual diagnosis evaluations and provides the structured, compassionate care that this particular combination of conditions requires.
You do not have to have hit a definable bottom. If your relationship with Xanax and your mood are making your life smaller than it should be, that is enough reason to reach out.
Contact Legacy Healing New Jersey confidentially at legacyhealingnj.com or call 516-928-6392. We are here when you are ready.



